fMRI Data PreprocessingWhat are the steps for preprocessing fMRI data?
|
|
Prior to subjecting raw fMRI data to any type of statistical analysis, most of the following pre-processing steps are commonly performed.
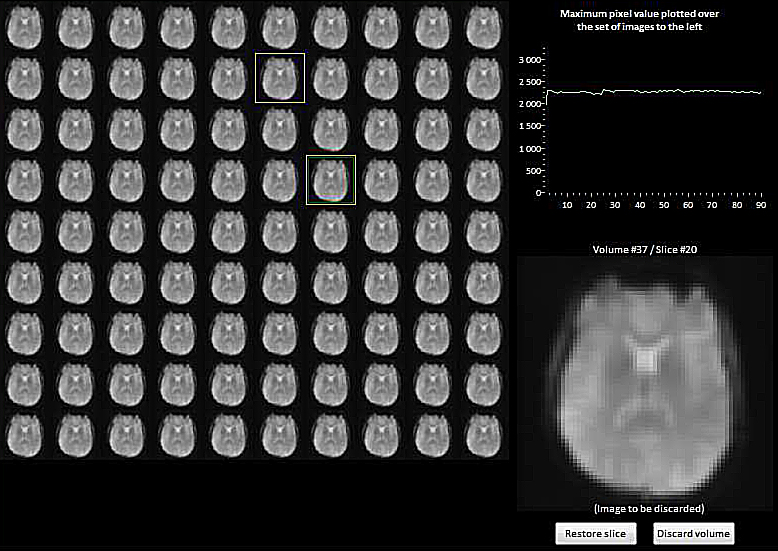 Montage view of source data from an fMRI series
Montage view of source data from an fMRI seriesallowing recognition and exclusion of aberrant individual slices
Quality Assurance: Inspection of source images. Individual slices in an fMRI acquisition commonly suffer from random variations in average signal intensity, noise spikes, ghosts, and data glitches. These may result from physiological sources (patient motion, respiration, cardiac pulsations, anxiety, drowsiness, drugs) or from the scanner itself (field inhomogeneities, eddy currents, gradient heating, electronics). If unrecognized and included in the data analysis, these may spoil the entire experiment. A quick visual review of all source images together in montage mode is highly recommended to search for and exclude ("scrub") aberrant slices that appear too bright, too dark, or contain artifacts. More sophisticated graphical and semi-automated methods to identify outlier data are also available.
|
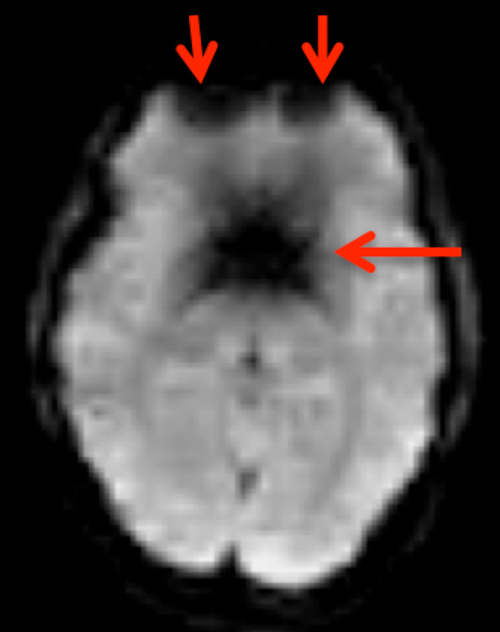
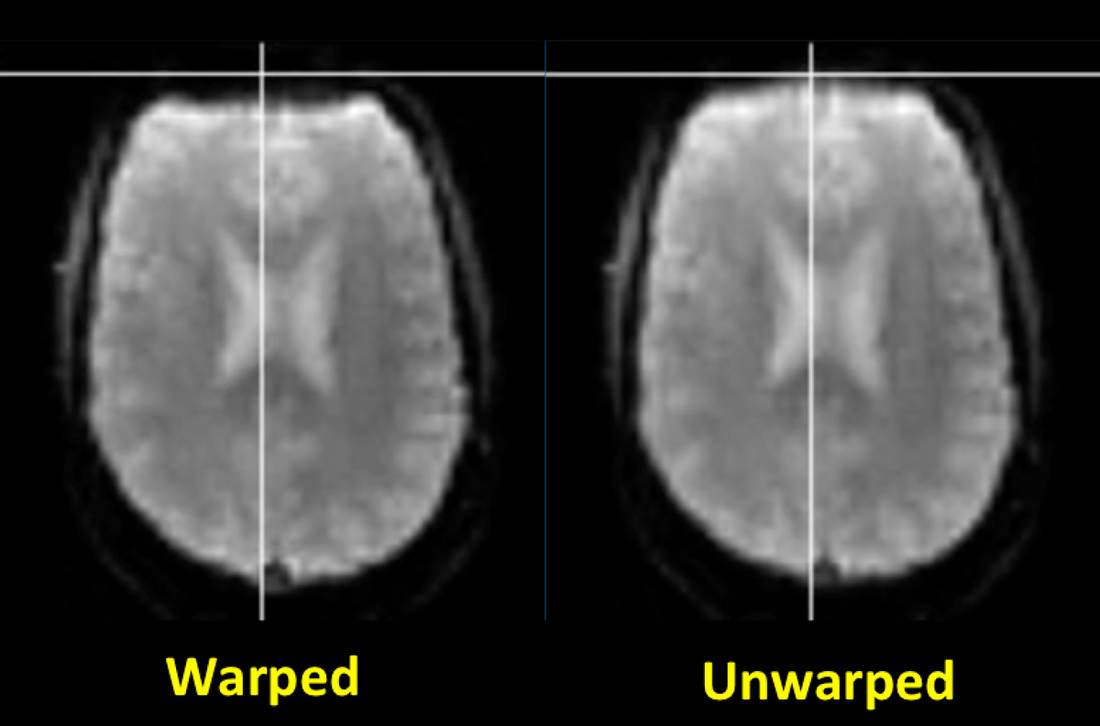
Distortion correction. Common fMRI/BOLD sequences acquire gradient echoes and hence are sensitive to magnetic inhomogeneity (T2*) effects. These cause spatial distortions and signal dropout especially near the skull base, typically affecting the anterior frontal and temporal lobes.
Field mapping and "unwarping" methods (described in the Advanced Discussion) are available to reduce these distortions. Although these techniques may be required for sophisticated neuropsychological experiments, they are not commonly used for basic eloquent cortex mapping in clinical fMRI studies. |
Slice timing correction. Most fMRI studies acquire one slice at a time, meaning that the signal recorded from one slice may be offset in time by up to several seconds when compared to another. The situation is even further complicated depending on whether the slices have been acquired in sequential (1,2,3,4,5,6...) or in interleaved (1,3,5,..2,4,6...) order and whether simultaneous multi-slice imaging has been employed. Although slice timing differences may not be important for simple block design experiments, they can impart considerable errors in rapid, event-related fMRI studies if not accounted for.
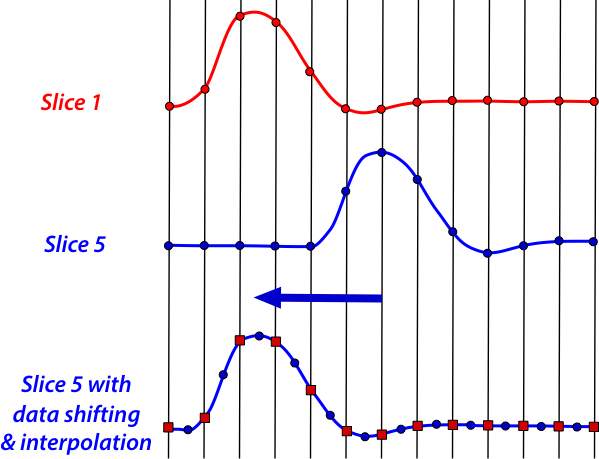
Two basic strategies have been developed for slice timing correction. Data shifting is the most commonly used method, where recorded points are moved to reflect their proper offset from the time of the stimulus. This method requires interpolation of points to fit the fixed, TR-based timing grid and thus produces some blurring and degradation of the data. An alternate (post-processing) strategy is model shifting, where the expected location of the hemodynamic response function (HRF) is varied, treating slice location as an additional independent variable in the subsequent statistical analysis. Sometimes temporal derivatives of the HRF are also incorporated in the model to improve accuracy.
 Residual mean-squared error
Residual mean-squared errorafter motion correction
Motion Correction. Head motion is the largest source of error in fMRI studies, and a variety of strategies have been developed to cope with this problem. Immobilization of the head using padding and straps is essential; even more rigid restrictions using bite bars and masks are occasionally employed. Proper coaching and training of the subject prior to imaging is important. Prospective motion correction using navigator echoes may be performed but more commonly motion correction is done retrospectively.
 Rotation and translation plots of the 6 parameters in a motion correction algorithm
Rotation and translation plots of the 6 parameters in a motion correction algorithmNote sudden head movement jump at acquisition #245. (Courtesy Chris Rorden)
The standard retrospective motion correction method considers the head as a rigid body with three directions of translation (displacement) and three axes of rotation. A single functional volume of a run is chosen as the reference to which runs in all other volumes are aligned. An iterative procedure is performed in which each volume is rotated and aligned with the reference, with the goal to minimize a cost function (such as the mean-squared difference). This iterative adjustment terminates once no further improvement can be achieved. All major fMRI analysis packages produce line plots allowing visual inspection of how translation and rotation parameters change from volume to volume (see figure above).
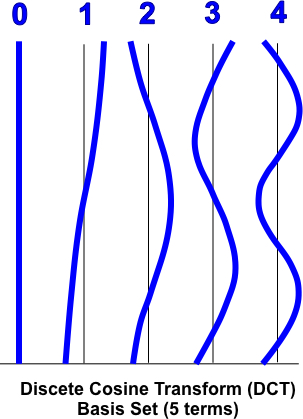
Temporal Filtering. fMRI data nearly always exhibit slow wandering of the baseline signal over time as well as rapid fluctuations due to noise. The removal of low frequency drifts is known as detrending. Detrending may be accomplished using either high-pass filtering after Fourier transformation or by time-domain averaging methods. Alternatively, gradual drifts can be removed later in the data analysis pipeline by adding a set of confound predictors (such as a discrete cosine transform basis set) to account for low-frequency fluctuations. High-frequency signal fluctuations (AKA "noise") can be removed by low-pass filtering. Low-pass filtering is generally not recommended for most studies, however, since it may distort estimation of individual HRFs and reduce the fMRI signals of interest.
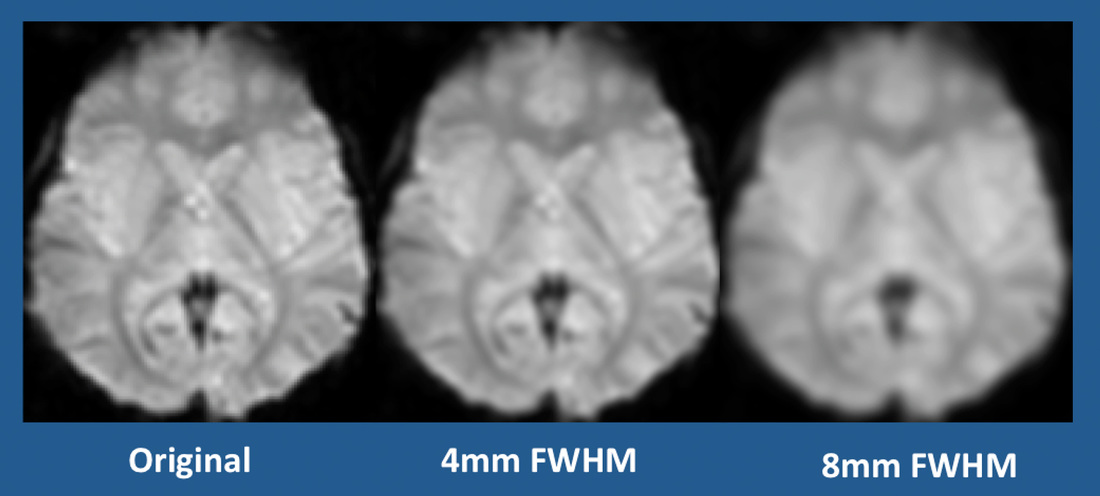 Spatial smoothing using Gaussian filters with various kernel widths
Spatial smoothing using Gaussian filters with various kernel widths(FWHM = full width half maximum)
Spatial Smoothing. Spatial smoothing is the averaging of signals from adjacent voxels. This improves the signal-to-noise ratio (SNR) but decreases spatial resolution, blurs the image, and smears activated areas into adjacent voxels. The process can be justified because closely neighboring brain voxels are usually inherently correlated in their function and blood supply. The standard method is to convolve ("multiply") the fMRI data with a 3D Gaussian kernel ("filter") that averages signals from neighboring voxels with weights that decrease with increasing distance from the target voxel. The optimal kernel size is disputed, depending on factors such as slice thickness and in-plane resolution and the need for spatial separation of small activation regions. In practice, the full width half maximum (FWHM) value of the Gaussian spatial filter is typically set to about 4-6 mm for single subject studies and to about 6-8 mm for multi-subject analyses.



References
Ashburner J, Friston KJ. Rigid body registration. In: Frackowiak RSJ (ed). Human Brain Function, 2nd ed. London: Academic Press, 2004. (pdf made available on-line by the authors at http://www.fil.ion.ucl.ac.uk/spm/doc/books/hbf2/)
Berman H, Mulders J, Goebel R. Anatabacus v1.1: Calculator for image distortions for Brain Voyager QX, 2014. (Detailed manual describing procedures for distortion correction using Brain Voyager, available from this link. Includes useful information about how to compute field maps and other practical measures for reducing susceptibility distortions.)
Chen JE, Glover GH. Functional magnetic imaging methods. Neuropsychol Rev 2015; 25:289-313.
Friston KJ, Josephs O, Zarahn E, et al. To smooth or not to smooth? Bias and efficiency in fMRI time-series analysis. NeuroImage 2000; 12: 196-208. (discussion of temporal smoothing, including bandpass filtering and whitening).
Maclaren J, Herbst M, Speck O, Zaitsev M. Prospective motion correction in brain imaging: a review. Magn Reson Med 2013; 69: 621–636.
Mikl M, Maraček R, Hluštík P, et al. Effects of spatial smoothing on fMRI group inferences. Magn Reson Imaging 2008; 26:490-503.
Sladky R, Friston KJ, Tröstl J, et al. Slice-timing effects and their correction in functional MRI. Neuroimage 2011; 58:588-594.
Tanabe J Miller D, Tregellas J, et al. Comparison of detrending methods for optimal fMRI preprocessing. NeuroImage 2002; 15:902–907.
The FIL Methods Group. SPM12 Manual. Welcome Trust Center for Neuroimaging, London, 2016. (describes preprocessing steps available in the SPM program).
Ashburner J, Friston KJ. Rigid body registration. In: Frackowiak RSJ (ed). Human Brain Function, 2nd ed. London: Academic Press, 2004. (pdf made available on-line by the authors at http://www.fil.ion.ucl.ac.uk/spm/doc/books/hbf2/)
Berman H, Mulders J, Goebel R. Anatabacus v1.1: Calculator for image distortions for Brain Voyager QX, 2014. (Detailed manual describing procedures for distortion correction using Brain Voyager, available from this link. Includes useful information about how to compute field maps and other practical measures for reducing susceptibility distortions.)
Chen JE, Glover GH. Functional magnetic imaging methods. Neuropsychol Rev 2015; 25:289-313.
Friston KJ, Josephs O, Zarahn E, et al. To smooth or not to smooth? Bias and efficiency in fMRI time-series analysis. NeuroImage 2000; 12: 196-208. (discussion of temporal smoothing, including bandpass filtering and whitening).
Maclaren J, Herbst M, Speck O, Zaitsev M. Prospective motion correction in brain imaging: a review. Magn Reson Med 2013; 69: 621–636.
Mikl M, Maraček R, Hluštík P, et al. Effects of spatial smoothing on fMRI group inferences. Magn Reson Imaging 2008; 26:490-503.
Sladky R, Friston KJ, Tröstl J, et al. Slice-timing effects and their correction in functional MRI. Neuroimage 2011; 58:588-594.
Tanabe J Miller D, Tregellas J, et al. Comparison of detrending methods for optimal fMRI preprocessing. NeuroImage 2002; 15:902–907.
The FIL Methods Group. SPM12 Manual. Welcome Trust Center for Neuroimaging, London, 2016. (describes preprocessing steps available in the SPM program).
Related Questions
How is fMRI data processed and analyzed?
How is fMRI data processed and analyzed?